Hemorrhoidal radiofrequency is a minimally invasive surgical technique/procedure recently used for the management of grade 2 and 3 mucohemorrhoidal prolapse, after failure of instrumental treatments.
We report the case of a patient whose hemorrhoidal radiofrequency procedure was complicated by perineal fasciitis
A 62-year-old man undergone a radiofrequency surgery for grade 4 hemorrhoidal prolapse. This patient had a history of overweight (weight 90kg for a height of 175cm, BMI = 29), type 2 diabetes evolving since 2019 unbalanced (HbA1c at 8%) and treated with metformin, hydrochloride + sitagliptin, and dapagliflozin 10mg per day, high blood pressure, coronary artery disease. The procedure took place with intraoperative antibiotic prophylaxis (metronidazole) without intraoperative complications. The total energy delivered was 3453 Joules for a duration of 2 min 20 seconds. A pudendal block with Ropivacaine 7.5mg/l 20ml had previously been performed.
The evolution was marked by an acute diarrhea under laxatives and chills. Two days later, he was admitted in intensive care unit for collapse and lactic acidosis (PH 7.27 lactate: 6.8 mmol / l). Clinical examination of the perineum noted a hematoma without ulceration or necrosis. Absence of dermo hypodermatitis or ulceration.
Biology: Leukocytes 9270/mm3, CRP at 644mg/l, creatinine 205 umol/l
Blood cultures, stool cultures and Clostridium difficile tests are negative.
The diagnosis of perineal fasciitis was mentioned. The CT scan found a significant infiltration of peri bladder, peri sigmoid and perineal fat (a). The antibiotic therapy prescribed was: piperacillin + tazobactam and clindamycin for 48 hours then piperacillin + tazobactam alone. Dapaglifozin was stopped 3 days after the onset of symptoms.
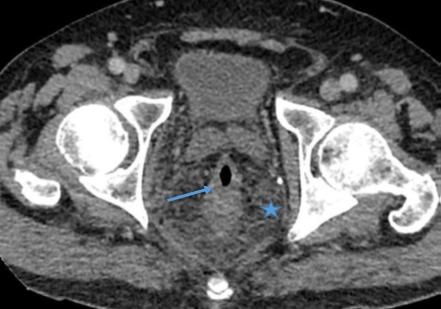

Figures 1 and 2 : CT scan with infiltration and enhancement of perirectal tissue (*), and thickening of rectal wall (->).
The rectosigmoidoscopy performed four days after the procedure shows a grayish appearance of the distal portion of the rectum without ulceration or necrosis. The mucosa appeared normal.
On the fifth postoperative day the patient remained subfebrile at 37 8 ° C and suffered from anal pain. The clinical examination finded an erythematous dermohypodermic infiltration of the two ischio fossa predominant on the left for about 12 cm with « cardboard » perception of the tissues. Absence of crackling or signs of gangrene. Absence of ulceration.
Biology: CRP 588, Leukocytes 8440/mm3, Creatinine 81umol/l, lactates 1.6mmol/l
The CT scan performed seven days after the procedure noted a thickening and a defect of parietal enhancement extending from the margin to the recto-sigmoid hinge with an infiltration of the peri-digestive and pre-sacral fat. Lack of collection.
The clinical course noted an improvement in cutaneous and subcutaneous infiltration on the right while left infiltration persists identical without regression.
The perineal MRI performed eleven days after the intervention noted a thickening of the wall of the rectum measured at 16mm without a clear abscess. Fluid infiltration of meso rectal fat collecting in presacral on 10 cm cranio caudal axis (b). In terms of antibiotic therapy, metronidazole and linezolid are added to piperacilline + tazobactam on the eleventh postoperative day.
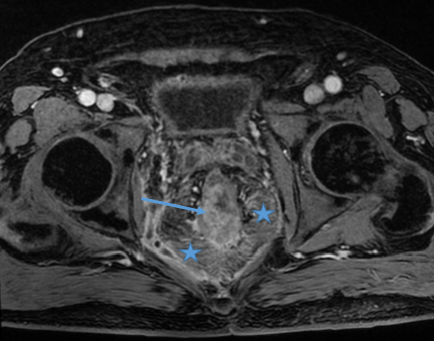
Figures 3 and 4: Pelvic MRI: T1 Weighted Fat supressed sequence with gadolinium injection, transversal plane: Infiltration and enhancement of perirectal tissus (*) with regular rectal wall thickness (->).

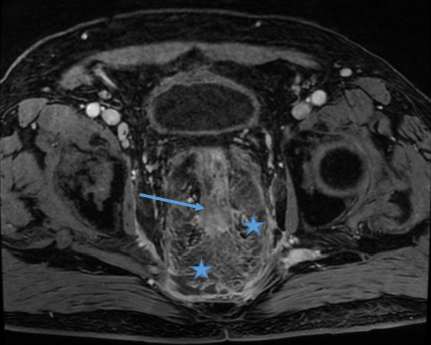
Figure 5: Pelvic MRI T1 Weighted Fat supressed sequence with gadolinium injection, transversal plane: Infiltration and enhancement of ischiorectal fossae fat (->).
A new rectosigmoidoscopy didn’t find mucosal abnormalities or signs of ischemia.
Three weeks after the procedure, the clinical course remained stable with left dermohypodermic infiltration without ulceration or necrosis.
A second control perineal MRI performed nineteen days after the intervention showed mesorectal infiltration about 16cm high with parietal thickening but regressing. Lack of collection and fistula communicating with the anal canal. Cytosteatonecrosis of ischiorectal fat without abscess.
We decided not to operate in the face of the absence of deterioration of the general condition and the local aspect which remained stable (absence of perineal necrosis, stability of the dermohypodermic lesion, absence of crepitations and absence of collection and fistulous path on medical imaging) during multi-daily clinical examinations.
The evolution was favorable under antibiotic therapy for 21 days and after discontinuation of dapagliflozin: complete regression of bilateral infiltration of the ischiorectal fossae and quasi-normalization of biological parameters 3 weeks after the intervention: CRP 29mg / l; leukocytes 6600/mm3; creatinine 51 umol/l. The patient returned home after three weeks of hospital monitoring. A weekly follow-up was carried out for one month. A normalization of biological parameters was achieved five weeks after the intervention.
Discussion
In this patient, Fournier’s gangrene, which is a rare complication but feared for any perineal procedure, was immediately suspected. The stable perineal clinical course without necrosis or gangrene under antibiotic therapy and despite perirectal infiltration, made it possible to avoid a wide surgical flattening. The diagnosis of perineal fasciitis without progression to gangrene was retained.
Fournier’s gangrene has an incidence of 1.6 cases per 100,000 men, with male predominance occurring preferentially after age 60. Known risk factors for Fournier’s gangrene are diabetes, overweight, vascular terrain, immunosuppression and some medications including sodium-glucose-2 cotransporter inhibitors (SGLT2). A perineal procedure is recognized as an input factor. (1, 2)
SGLT 2 is an antidiabetic treatment also used to improve cardiac failure and renal failure. This class of antidiabetic treatment increases urinary sugar excretion and so lowers blood sugar. This urinary excretion would promote bacterial proliferation in the urogenital tract as well as a ketoacidosis.
The Food and Drug Administration issued a warning in 2018, repeated in 2020 about 55 cases of Fournier’s gangrene reported between 2013 and 2019, potentially related to the use of SGLT 2. A recent study cited 542 cases including 86 cases on dapagliflozin and 12 cases on dapagliflozin and metformin (3,4)
However, a causal relationship between SGLT2 and Fournier’s gangrene is not demonstrated in a recent study comparing the incidence of Fournier’s gangrene between two classes of antidiabetic medications: SGLT2 vs gliptin (5)
More recently, 5 cases of Fournier’s gangrene potentially linked to dapagliflozin were reported. All cases were male. One had a history of radiotherapy of the perineal sphere and a second urinary invasive procedures. The other three patients had no perineal history. (6)
A meta-analysis found a link between the different SGLT2 specialties and genital infections but not with urinary tract infections. Only dapagliflozin at a dose of 10mg per day maintained this link with urinary tract infections (7)
Minor (11.2%) and severe (8.2%) complications are reported after hemorrhoidal radiofrequency. The latter complications are per or postoperative hemorrhagic complications, severe pain, hyperthermia and 2 patients with hemorrhoidal ulceration of favorable evolution. To our knowledge, severe perineal sepsis has not yet been reported. (8,9)
Radiofrequency can lead to ulcerations of hemorrhoidal tissue that can potentially promote perineal suppuration. Our patient had never clinically presented ulcer or necrosis of treated hemorrhoidal packets. It should be noted that the operating procedure had respected the recommendations of energy delivered. In conclusion, this is the first case of severe septic complication after hemorrhoidal radiofrequency. This procedure is present as a minimally invasive surgical technique with only minimal complications reported. Our patient has the classic risk factors for Fournier’s gangrene. Taking a treatment of dapaglifozin, recently recognized as the cause of such complications, should be taken into consideration when a proctological intervention is considered even if it’s a minimally invasive surgical procedure.
Conclusion
Cette classe thérapeutique est de plus en plus souvent rencontrée car prescrite pour un diabète, et aussi chez les insuffisants cardiaques. Chez ces patients, les indications des gestes invasifs proctologiques instrumentaux ou chirurgicaux doivent tenir compte du risque potentiellement augmenté de complication infectieuse. Si un patient sous dapagliflozine présente un sepsis périnéal, il est conseillé d’arrêter ce traitement.
Références
- Lewis G D, Majeed M, Olang C A, et al. (October 21, 2021) Fournier’s Gangrene Diagnosis and Treatment: A Systematic Review. Cureus 13(10): e18948 https:// doi 10.7759/cureus.18948
- Houdeville C, Egal A, Meyssonier V Etienney I. la cellulite pelvienne/ une urgence médicochirurgicale. Hepato-Gastro et OncologieDigestive 2021 ; 28 : 377-382.https:// doi .org/10-1684/hpg.2021.2148
- FDA. Fda warns about rare occurrences of a serious infection of the genital area with SGLT2 inhibitors for diabetes, 2018. https://www.fda.gov/Drugs/DrugSafety/ucm617360.htm
- Hu Y, Bai Z, Tang Y, et al. Fournier Gangrene Associated with Sodium-Glucose Cotransporter-2 Inhibitors: A Pharmacovigilance Study with Data from the U.S. FDA Adverse Event Reporting System. Journal of Diabetes Research Volume 2020, Article ID 3695101, 8 pages https://doi.org/10.1155/2020/3695101
- Yang JY, Wang T, Pate V, et al. Real-world evidence on sodium-glucose cotransporter-2 inhibitor use and risk of Fournier’s gangrene. BMJ Open Diab Res Care 2020;8:e000985. https://doi.org10.1136/ bmjdrc-2019-000985
- Elbeddini A, Tayefehchamani Y, Davey M, et al. Fournier’s gangrene with dapaglifozin in a rural hospital: a case report. BMJ Case Rep 202 ; 14 :e237784https:// doi.org/10.1136/bcr-2020- 237784
- Puckrin R, Saltiel MP, Reynier P, et al. SGLT-2 inhibitors and the risk of infections: a systematic review and meta-analysis of randomized controlled trials. Acta Diabetol 55, 503–514 (2018). https://doi.org/10.1007/s00592-018-1116-0
- Didelot JM, Raux B, Didelot R, et al. What can patients expect in the long term from radiofrequency thermocoagulation of hemorrhoids on bleeding, prolapse, quality of life, and recurrence: “no pain, no gain” or “no pain but a gain”? Ann Coloproctol 2022 Oct 11 [Epub ahead of print] https: //doi.org/10.3393/ac.2022.00311.0044
- Tolksdorf S, Tübergen D, Vivaldi C, et al. Early and midterm results of radiofrequency ablation (Rafaelo® procedure) for third-degree haemorrhoids: a prospective, two centre study. Tech Coloproctol 2022;26:479-87. https://doi.or/10.1007/s10151-022-02608-x